
Inventory management has become a key focus at all healthcare providers as a result of the Affordable Care Act (ACA) and an ever-increasing need for operating capital.
In the past, providers have turned to a consignment strategy for infrequently used but very expensive items like catheters, stents, and heart defibrillators. However, consignment practices in healthcare are really a strange deal. Not only do these practices include the complexities of the change of ownership inherent to consignment, they also utilize a disconnected vendor managed inventory (VMI) approach.
Why is this concerning? Hospitals are now putting some of the most expensive inventory in the hands of people who directly manage your stock and have the ability to invoice directly. Yet, it is very common for materials managers to say consignment offerings do not require them to track the inventory with the same scrutiny as owned inventory. Everyone in the chain of command will probably disagree out of principle, but no one is trying to do much about it.
Imagine if we told the CFO that consignment vendors have little to no oversight or independent auditability. The statement is probably not a good conversation starter. The frugal climate created by ACA and competing incentive packages for vendor reps are completely at odds. As a result, the motivation for fraud to occur can only go up.
Healthcare is spending millions on ERP, MMIS, Lean, Kanban, and other inventory management technologies, and yet we still think consignment and third party management of the inventory is sustainable. It could be sustainable if the vendor is fully integrated into the inventory process, but typically they are not.
Fraud is Real
Before you immediately say: “oh, we don’t have fraud,” you are really just lying to yourselves. Here are just a few examples of fraud taking place as a result of consignment practices in healthcare.
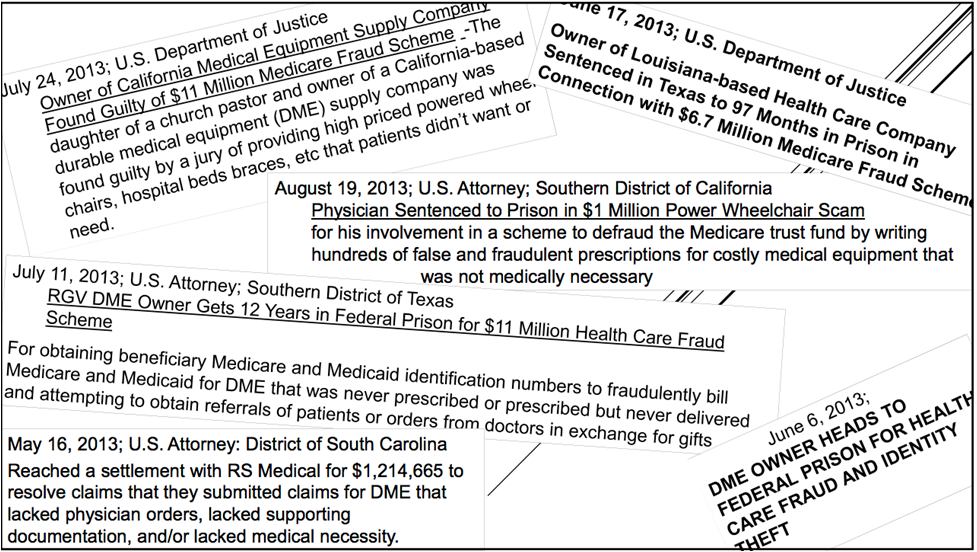
Image Credit: Robert Hussar, Esq., CHC Manatt, Phelps & Phillips, LLP 30 S. Pearl Street Albany, NY 12207 (518) 431-6730 rhussar@manatt.com Jack Pivar General Counsel Numotion (518)475-0837 jackpivar@JJPhealthlawyer.com
People Are Human and Tensions Keep Mounting
Medical implant and device vendors employ salespeople who are paid based on the amount of product used by hospitals. Because of ACA, there are mounting tensions among physicians, surgeons, materials managers, and vendors.
Physicians and surgeons have relationships with suppliers who they feel provide the best products to care for their patients. Materials managers are trying to contain costs based on tightening budgets. Vendors are looking to maximize their revenue. With these conflicting motivations someone is going to get pinched in the process. Most likely that would be the vendors.
We Aren’t Talking Bread and Bicycles
What do bread and bicycles have to do with this conversation? In a pair of articles by Dave Piasecki, Owner of Inventory Operations, LLC, he uses bread and bicycles for examples of Consignment and Vendor Managed Inventory (VMI).
Bread is provided to restaurants and grocery stores by the local Wonder Bread guy who looks at the inventory, stocks it back up, and bills you for the difference. This is an example of consignment and VMI together. Consignment is only paying for what is used, and VMI is allowing the vendor to control restocking.
In the case of bicycles, a bike store is not going to invest in inventory that does not have a proven track record of sales. So the store may display the bicycle for a vendor in their retail space without actually paying for it. This example is really just consignment by itself.
How are medical implants and devices different? Bread is quite bulky and very inexpensive, and bicycles are very expensive and extremely awkward. Ranging from $3,000-$30,000, medical implants and devices like stents, mesh, or defibrillators have a great range of sizes and values. Most of it though is quite small. Products could be moved from hospital to hospital very easily if there are not strong inventory management policies and vendor auditing in place.
Consignment Gone Wrong
Inventory management is already a pain in the butt with the sheer number of SKUs, surgeon preferences, irregular usage patterns, etc. Add to that a completely separate process for tracking vendor managed consignment, and you have the makings of even more murkiness in the supply chain.
Let’s walk through a worst-case scenario. You have a vendor rep that regularly restocks items in Cath Lab. Often this product will coexist with the same product that has already been purchased by the hospital. Why would the hospital have the same product for both owned and consigned inventory? Because somebody in purchasing got hit up with a sweet end of quarter deal on catheters and bought them in bulk. Now maybe only the coordinator in charge of the Cath Lab knows what is consigned and not consigned. If this employee leaves or gets hit by a bus, there are potentially tens of thousands of dollars of losses in not being able to identify consigned versus not consigned items during procedure.
You also have a team executing periodic inventory in the Cath Lab, but the vendor rep is keeping track of consignment on a separate Excel spreadsheet. If the team doing the periodic inventory does not know the difference between the owned and consignment items, they can very easily overstate the value of your inventory. Obviously having separate processes for owned and consigned inventory could lead to inconsistencies which ultimately cause discrepancies in inventory valuations.
Let’s go back to the Excel spreadsheet used by the vendor. The rep uses that same spreadsheet to create invoices. The hospital in most cases never sees the rep’s inventory count except when the hospital sends a request to the rep to get the inventory on-hand. Now here is the problem of incentives. The hospital got a sweet deal on the catheters. You would like to burn down that inventory before it is expired or becomes obsolete. The rep wants the hospital to use his catheters, resulting in commissions for him. If he is being asked what the inventory count is, what is to stop him from shorting the count? People are human, and this type of scenario is one that could lead to the fraud cases everyone is seeing.
What Can You Do?
There are a lot of obvious steps that we can take to fix this problem; however, this problem is a direct result of the minor details that are often overlooked.
First, hospitals need to take control of the relationship with the vendors. Too often hospitals work from consignment contracts that are provided by the vendor. The hospital should institute standard consignment policies and contracts to govern their relationships. These contracts should be easily accessible by all parties within the hospital supply chain.
Second, hospitals should be implementing their standard inventory management policies with the vendor. The vendor should be subject to audits and required to utilize the hospital’s inventory management technology.
Third, all consignment items should be part of the item master within the financial system so that it can be reconciled against invoices provided by the vendor.
Finally, because the margins on these products are so high (up to 90%), hospitals should be putting more pressure on vendors to have a distribution system that more closely resembles just-in-time practices.
You Have Been Warned
Consignment and vendor managed inventory practices need to be transparent to realize the cost savings benefits you would hope to get from using the practices. Otherwise, you leave yourself open to potential fraud and abuse which will absolutely negate all the savings you believed you were receiving.